Ear pulling, restless nights, and unexplained crying often point to an ear infection. They are one of the most common reasons young children visit the doctor.
Most cases clear up on their own or with a short course of antibiotics. Knowing the symptoms, causes, and treatment options helps you decide when home care is enough and when to book an appointment.
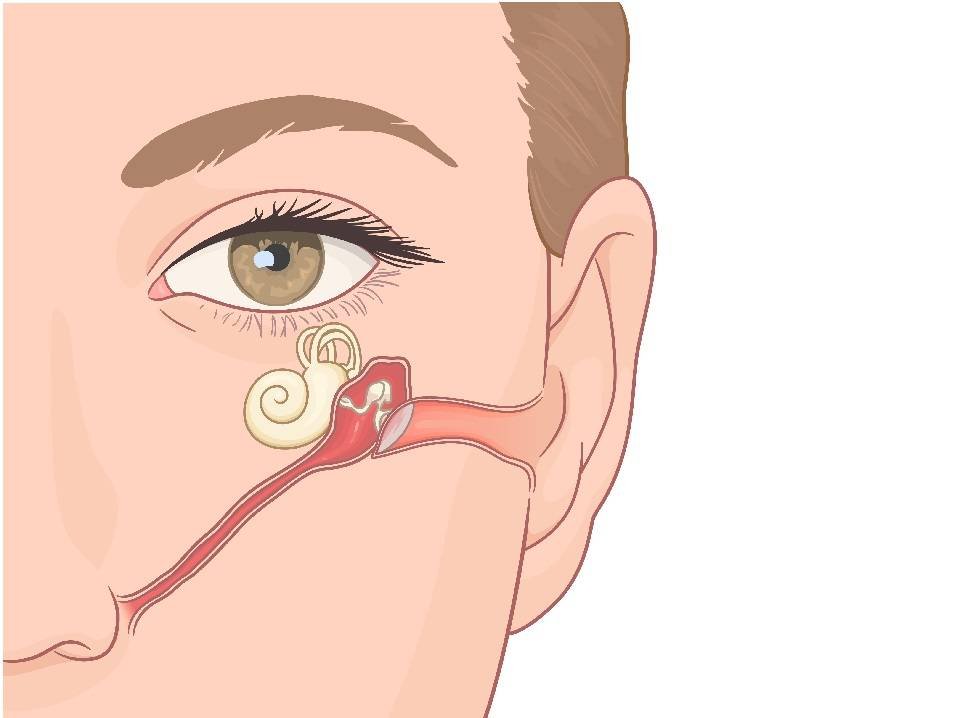
Otitis Media: Infection Behind the Eardrum
Ear infections (otitis media) happen when the middle ear becomes inflamed. Bacteria or viruses reach the middle ear through the Eustachian tube.
The Eustachian tube connects the middle ear to the back of the throat.
About 5 in 6 children have at least one ear infection by age 3, per the American Academy of Pediatrics.
Boys develop ear infections slightly more often than girls.
What Raises the Risk in Babies and Toddlers
Infections often spread from the nose or throat into the middle ear. Other risk factors include:
Secondhand smoke irritates the Eustachian tube and increases mucus, which blocks drainage.
Keep smoke away from your child indoors and in cars.
Allergies inflame nasal passages and block the tube. A skin prick allergy test can identify triggers in children.
Colds and respiratory infections cause congestion that opens the door to middle-ear infection.
Bottle-feeding and pacifiers may affect Eustachian tube function compared with breastfeeding, though many bottle-fed babies never develop chronic ear problems.
Daycare exposure and family history also increase frequency.
AOM vs OME: Two Types Parents Hear About
- Acute otitis media (AOM): Sudden ear pain, fever, and irritability. Often bacterial, sometimes with fluid behind the eardrum.
- Otitis media with effusion (OME): Fluid remains after AOM without strong pain. Easy to miss. Untreated OME can affect hearing.
Symptoms to Watch For
Ear pain: Pulling at ears, crying, trouble sleeping. Some children, especially with OME, show little pain.
Fever and irritability: Track temperature with a thermometer. Poor feeding or restlessness often accompany fever.
Drainage: Clear, yellow, or bloody fluid may mean a ruptured eardrum. Seek medical attention if you see drainage.
How Doctors Diagnose Ear Infections
A clinician examines the ear canal and eardrum with an otoscope, looking for bulging, redness, or fluid.
Swabs or hearing tests (tympanometry, audiometry) are used when diagnosis is unclear or hearing is a concern.
Treatment: Watchful Waiting, Antibiotics, and Surgery
Watchful waiting suits mild cases or OME. Pain relief and monitoring may be enough.
Antibiotics treat confirmed bacterial AOM, especially with severe symptoms or complications. Finish the full course prescribed.
Ear tubes are reserved for chronic or recurrent infections that affect hearing or quality of life.
Pain relievers (acetaminophen or ibuprofen) reduce pain and fever. Follow age- and weight-based dosing.
Ear drops may be prescribed for pain or inflammation. Use only as directed.
Home Comfort Measures (Not a Substitute for Care)
A warm compress on the outer ear can ease discomfort.
Some families use garlic oil drops; discuss any home remedy with your paediatrician first. These support comfort but do not replace medical treatment when infection is confirmed.
Prevention: Hygiene, Vaccines, and Breastfeeding
Wash hands before feeding or touching your child's face.
Keep vaccinations current, including pneumococcal and annual flu vaccine, per the Singapore immunisation schedule. Vaccines lower risk of respiratory illness that leads to ear infections. See our child immunisation guide for timing details.
Breastfeeding, when possible, supports immune defences and healthy gut bacteria linked to fewer infections.
Avoid secondhand smoke and treat allergies promptly.
When to See a Doctor Urgently
- Symptoms persist or worsen after 48 to 72 hours of home care
- High fever, severe pain, or hearing difficulty
- Fluid draining from the ear
- Frequent repeat infections
Complications If Infections Go Untreated
Repeated or untreated infections can cause temporary hearing loss, speech delays, and chronic middle-ear fluid. Early treatment protects development.
Follow-Up and Long-Term Care
Most ear infections resolve without lasting harm. If episodes keep returning, a paediatrician can check for underlying causes and discuss ear tubes or other options.
For related reading, see fever in toddlers and common childhood illnesses.